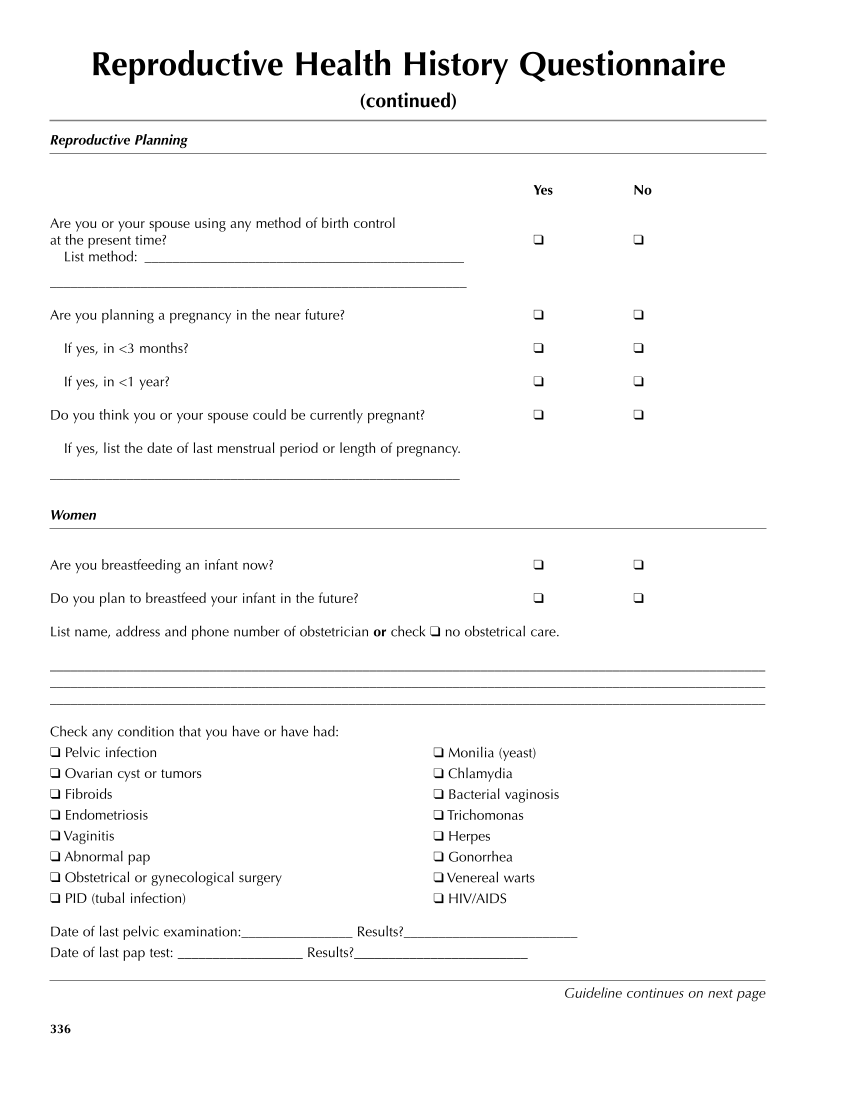
Reproductive Health History Questionnaire (continued) Reproductive Planning Yes No Are you or your spouse using any method of birth control at the present time? ❑ ❑ List method: ______________________________________________ ____________________________________________________________ Are you planning a pregnancy in the near future? ❑ ❑ If yes, in 3 months? ❑ ❑ If yes, in 1 year? ❑ ❑ Do you think you or your spouse could be currently pregnant? ❑ ❑ If yes, list the date of last menstrual period or length of pregnancy. ___________________________________________________________ Women Are you breastfeeding an infant now? ❑ ❑ Do you plan to breastfeed your infant in the future? ❑ ❑ List name, address and phone number of obstetrician or check ❑ no obstetrical care. _______________________________________________________________________________________________________ _______________________________________________________________________________________________________ _______________________________________________________________________________________________________ Check any condition that you have or have had: ❑ Pelvic infection ❑ Ovarian cyst or tumors ❑ Fibroids ❑ Endometriosis ❑ Vaginitis ❑ Abnormal pap ❑ Obstetrical or gynecological surgery ❑ PID (tubal infection) Date of last pelvic examination:________________ Results?_________________________ Date of last pap test: __________________ Results?_________________________ 336 ❑ Monilia (yeast) ❑ Chlamydia ❑ Bacterial vaginosis ❑ Trichomonas ❑ Herpes ❑ Gonorrhea ❑ Venereal warts ❑ HIV/AIDS Guideline continues on next page
Purchased from OEM Press by (ge corporate access). (C) 2013 OEM Health Information, Inc. All rights reserved.