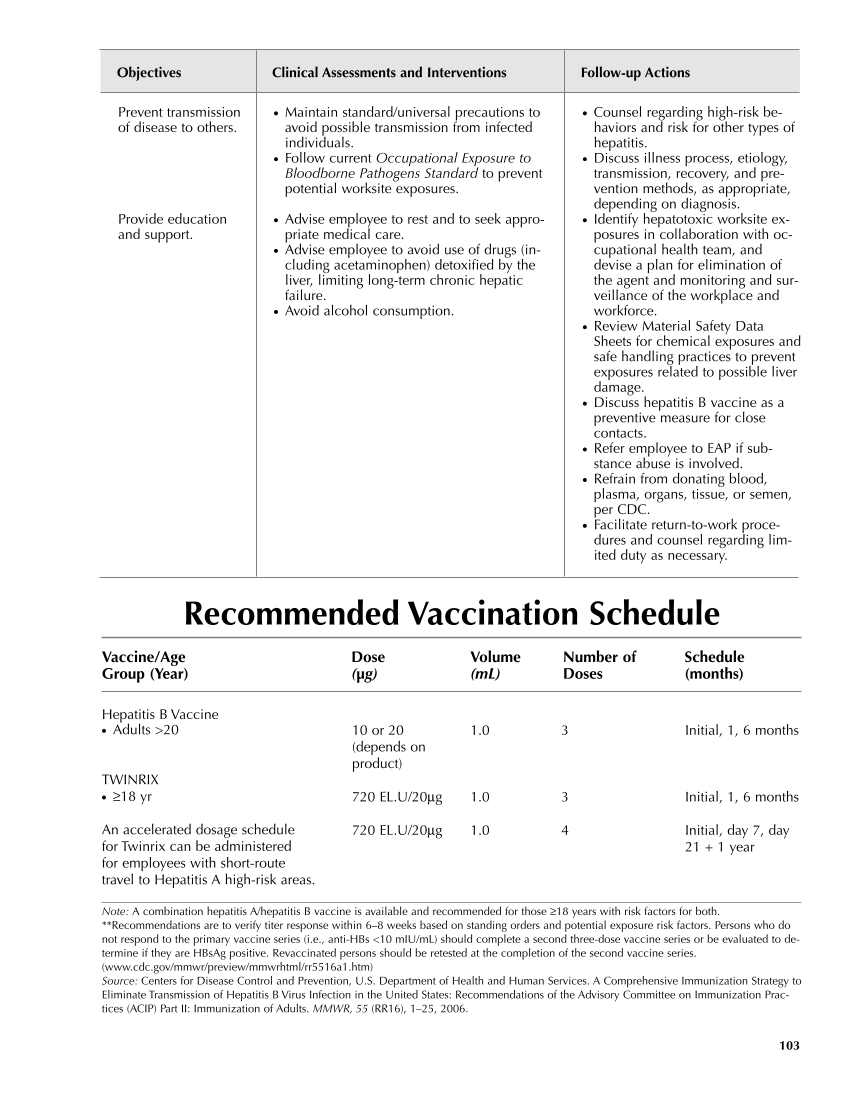
● Counsel regarding high-risk be- haviors and risk for other types of hepatitis. ● Discuss illness process, etiology, transmission, recovery, and pre- vention methods, as appropriate, depending on diagnosis. ● Identify hepatotoxic worksite ex- posures in collaboration with oc- cupational health team, and devise a plan for elimination of the agent and monitoring and sur- veillance of the workplace and workforce. ● Review Material Safety Data Sheets for chemical exposures and safe handling practices to prevent exposures related to possible liver damage. ● Discuss hepatitis B vaccine as a preventive measure for close contacts. ● Refer employee to EAP if sub- stance abuse is involved. ● Refrain from donating blood, plasma, organs, tissue, or semen, per CDC. ● Facilitate return-to-work proce- dures and counsel regarding lim- ited duty as necessary. Objectives Clinical Assessments and Interventions Follow-up Actions 103 Prevent transmission of disease to others. Provide education and support. ● Maintain standard/universal precautions to avoid possible transmission from infected individuals. ● Follow current Occupational Exposure to Bloodborne Pathogens Standard to prevent potential worksite exposures. ● Advise employee to rest and to seek appro- priate medical care. ● Advise employee to avoid use of drugs (in- cluding acetaminophen) detoxified by the liver, limiting long-term chronic hepatic failure. ● Avoid alcohol consumption. Recommended Vaccination Schedule Vaccine/Age Dose Volume Number of Schedule Group (Year) (μg) (mL) Doses (months) Hepatitis B Vaccine ● Adults 20 TWINRIX ● ≥18 yr An accelerated dosage schedule for Twinrix can be administered for employees with short-route travel to Hepatitis A high-risk areas. 10 or 20 (depends on product) 720 EL.U/20μg 720 EL.U/20μg 1.0 1.0 1.0 3 3 4 Initial, 1, 6 months Initial, 1, 6 months Initial, day 7, day 21 + 1 year Note: A combination hepatitis A/hepatitis B vaccine is available and recommended for those ≥18 years with risk factors for both. **Recommendations are to verify titer response within 6–8 weeks based on standing orders and potential exposure risk factors. Persons who do not respond to the primary vaccine series (i.e., anti-HBs 10 mIU/mL) should complete a second three-dose vaccine series or be evaluated to de- termine if they are HBsAg positive. Revaccinated persons should be retested at the completion of the second vaccine series. (www.cdc.gov/mmwr/preview/mmwrhtml/rr5516a1.htm) Source: Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. A Comprehensive Immunization Strategy to Eliminate Transmission of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Prac- tices (ACIP) Part II: Immunization of Adults. MMWR, 55 (RR16), 1–25, 2006.
Purchased from OEM Press by (ge corporate access). (C) 2013 OEM Health Information, Inc. All rights reserved.