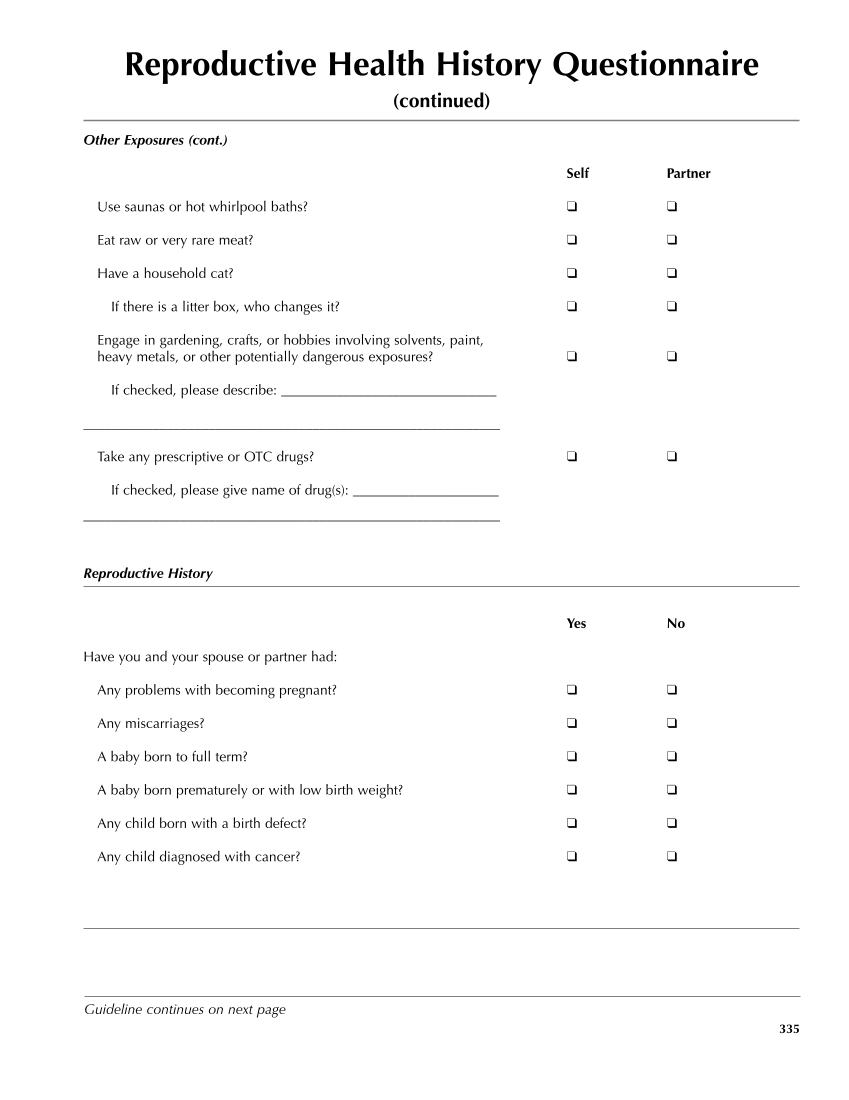
Reproductive Health History Questionnaire (continued) Other Exposures (cont.) Self Partner Use saunas or hot whirlpool baths? ❑ ❑ Eat raw or very rare meat? ❑ ❑ Have a household cat? ❑ ❑ If there is a litter box, who changes it? ❑ ❑ Engage in gardening, crafts, or hobbies involving solvents, paint, heavy metals, or other potentially dangerous exposures? ❑ ❑ If checked, please describe: _______________________________ ____________________________________________________________ Take any prescriptive or OTC drugs? ❑ ❑ If checked, please give name of drug(s): _____________________ ____________________________________________________________ Reproductive History Yes No Have you and your spouse or partner had: Any problems with becoming pregnant? ❑ ❑ Any miscarriages? ❑ ❑ A baby born to full term? ❑ ❑ A baby born prematurely or with low birth weight? ❑ ❑ Any child born with a birth defect? ❑ ❑ Any child diagnosed with cancer? ❑ ❑ 335 Guideline continues on next page
Purchased from OEM Press by (ge corporate access). (C) 2013 OEM Health Information, Inc. All rights reserved.